The practical story behind 3d printing medical devices is no longer about prototypes on a lab bench. In the U.S., the technology now supports patient-specific guides, prosthetics, dental parts, and selected implants when fit, geometry, and validation justify the workflow. I will walk through where it already works, how the digital-to-physical process really runs, what the FDA expects in 2026, and the limits that still matter more than the printer brand.
The practical takeaways that matter before you start printing
- Best fit: Additive manufacturing is strongest where a part must be custom, geometrically complex, or produced in low volume.
- Workflow matters: Imaging, segmentation, build orientation, post-processing, and verification shape the outcome as much as the printer does.
- U.S. rules changed in 2026: The FDA’s Quality Management System Regulation became effective on February 2, 2026 and now incorporates ISO 13485:2016 by reference.
- Material choice is not generic: Biocompatibility, load, sterilization, and intended contact determine whether a polymer or metal is appropriate.
- Most failures are process failures: Weak validation and poor traceability cause more trouble than the machine itself.
Why 3D printing matters in medical manufacturing
What makes additive manufacturing useful in medicine is not novelty. It is control. A digital file can be translated into a part that follows a patient’s anatomy, a surgeon’s plan, or a very specific mechanical requirement without forcing the design to fit a mold, a cutting tool, or a one-size-fits-all inventory model.
I tend to think of it as a way to remove unnecessary compromise. Traditional manufacturing is excellent when you want scale and repeatability. 3D printing becomes valuable when geometry, personalization, or internal structure matters more than raw volume. That is why it keeps showing up in places like surgical planning, orthotics, dental work, and implants with complex surfaces or lattice structures. The real question is not whether the part can be printed, but whether printing creates a better medical result.
That distinction becomes clearer when you look at the device categories where the technology already earns its keep.
Where it already works best
The strongest use cases are the ones where a custom shape changes the clinical workflow or the patient experience. I would group them into a few broad categories rather than treat every printed object as the same kind of medical product.
| Device category | Why 3D printing fits | Typical watch-out |
|---|---|---|
| Surgical guides and anatomical models | They can match patient imaging closely and help surgeons rehearse a procedure before entering the operating room. | Imaging errors, segmentation mistakes, and the need to define whether the model is for planning, communication, or direct clinical use. |
| Dental parts and restorations | Small parts, fine detail, and repeatable geometry are a natural fit for additive workflows. | Resin qualification, post-curing, wear resistance, and surface finish all matter more than many teams expect. |
| Orthopedic, cranial, and spinal implants | Patient-specific fit and porous or lattice structures can improve fixation and, in some cases, support osseointegration. | Fatigue strength, long-term stability, and a much higher validation burden than most prototypes require. |
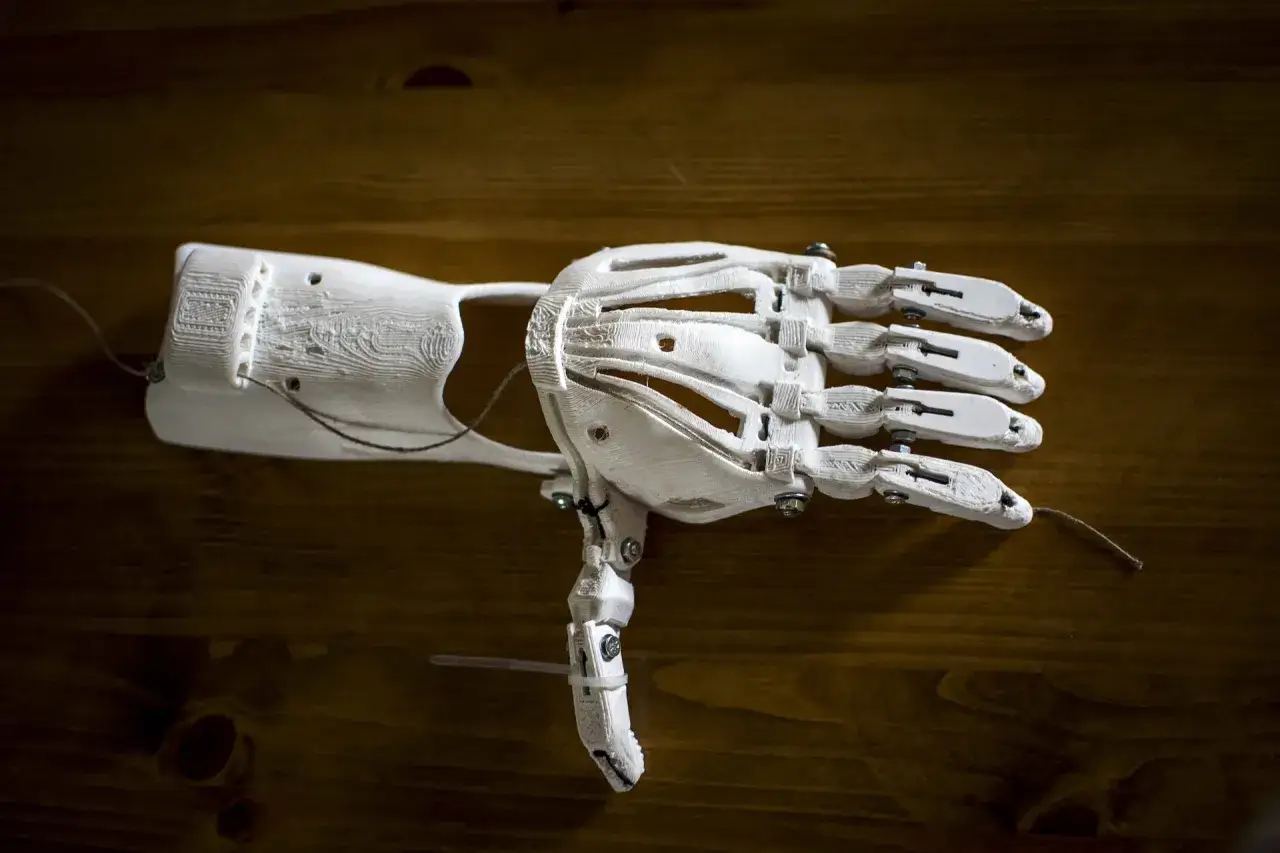
| External prosthetics and orthotics | Comfort, fit, and lighter-weight shapes can be customized quickly for a specific user. | Skin contact, durability, and finish quality are not optional details. |
| Instruments and fixtures | Complex handles, guides, or low-volume tools can be produced without expensive tooling. | Cleaning, sterilization, and repeated use can expose weak material choices quickly. |
The FDA notes that additive manufacturing has become the preferred manufacturing method for hearing aids and metal spine cages, which tells me the technology is already mature in some product lines and still evolving in others. That is the pattern to watch: where the part needs customization or internal complexity, the technology usually has a real advantage.
Once the use case is clear, the next question is how the digital file becomes a part that can actually be trusted.
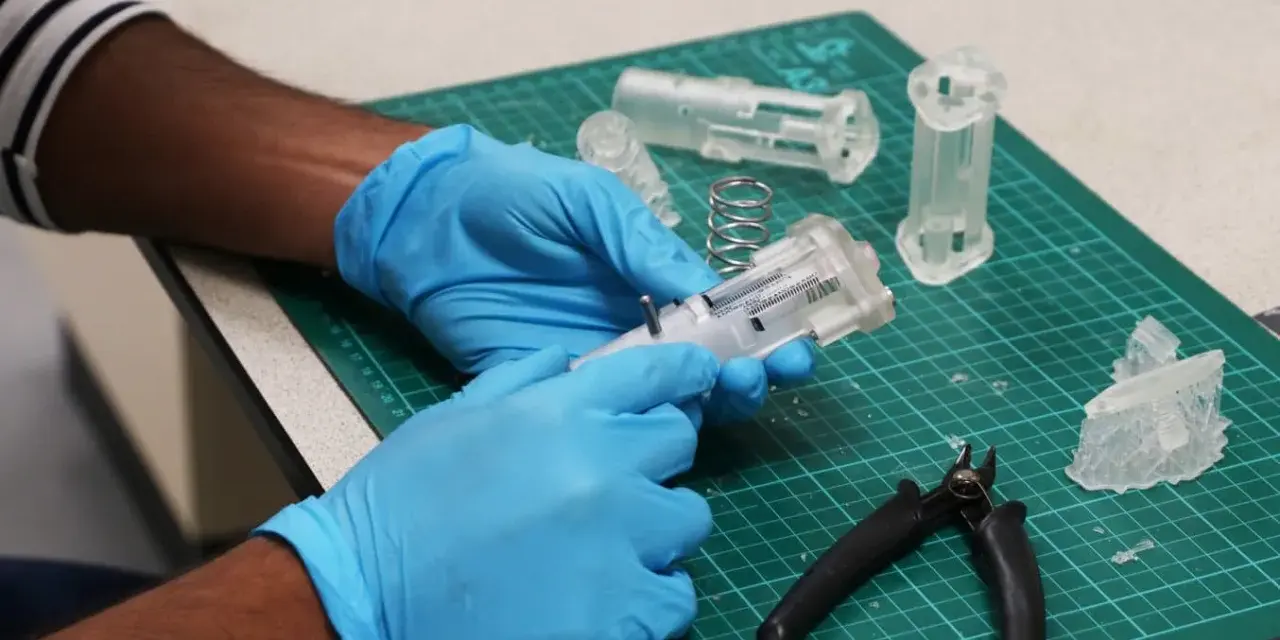
How a scan becomes a usable device
I do not think of the printing step as the whole process. In medical manufacturing, the printer is only one link in a chain that starts with imaging and ends with release for clinical use. If any link is weak, the part may still look good but fail where it counts.
- Imaging and segmentation: CT, MRI, or other imaging data is translated into a digital model. Segmentation is the part where anatomy is isolated from surrounding tissue or noise, and this step can make or break fit.
- Design for additive manufacturing: The part is adapted for printing, not just modeled for appearance. DfAM means designing for wall thickness, support removal, surface finish, and how the part will actually be cleaned or assembled.
- Build preparation: Orientation, supports, and layer strategy are set before printing starts. Build orientation matters because strength, surface quality, and dimensional accuracy can change depending on direction.
- Printing: The printer builds the object layer by layer under controlled parameters. This is where material behavior, machine calibration, and environmental control start to matter together.
- Post-processing: Cleaning, depowdering, curing, annealing, polishing, machining, or drilling may be needed. This is not cosmetic work; it often decides whether the part meets specification.
- Verification and sterilization: The finished part is inspected, tested, and sterilized if needed before release. For patient-contact devices, this is where dimensional stability and surface integrity must hold up.
If I had to name one common mistake, it would be treating post-processing like cleanup instead of manufacturing. That is where tolerances can drift, surfaces can change, and assumptions about safety can quietly fall apart. The next step is choosing the right process, because not every printer class is suitable for every medical job.
Choosing the right printing method for the job
The printer type matters, but only because each process comes with its own strength profile, surface quality, material options, and validation burden. I would never choose a process based on hype alone.
| Process | Best fit | Strengths | Main limits |
|---|---|---|---|
| FDM/FFF | Prototypes, fixtures, training models, and some noncritical patient-specific parts | Low cost, fast iteration, broad material availability | Visible layer lines, lower detail, and anisotropy, meaning strength can vary by build direction |
| SLA/DLP | Fine-detail models, surgical guides, and dental applications | High resolution, smooth surfaces, good small-part accuracy | Resin handling, post-curing, and sterilization constraints |
| SLS | Functional polymer parts, orthotics, and durable housings | No support structures, strong nylon parts, good design freedom | Powder cleanup, surface roughness, and tighter process control |
| Metal powder-bed fusion | Load-bearing implants and complex metal geometry | Excellent for lattices, porous surfaces, and high-performance metal parts | High cost, complex validation, and significant monitoring requirements |
For plastic medical parts, I pay special attention to whether the material is a medical-grade resin, a nylon, or a high-performance thermoplastic such as PEEK. Biocompatibility means the material has to behave safely for the intended contact type, not just look medical. Topology optimization, which means removing material where it does not add useful strength, can be powerful in implants, but it also raises the bar for testing and repeatability.
Method choice is really a trade-off between geometry, strength, surface quality, and how much proof the final part will need. That leads directly to the U.S. regulatory side, where the part’s intended use matters just as much as the printer.
What the FDA expects in the United States
In the U.S., printed medical products are not exempt from the normal device framework just because they come off an additive system. The FDA treats them as finished medical devices, and the rules are still built around intended use, risk, and quality control. The difference is that additive workflows add more variables that have to be documented and controlled.
The current landscape matters even more in 2026 because the FDA’s Quality Management System Regulation became effective on February 2, 2026 and incorporates ISO 13485:2016 by reference. In plain English, that means device makers need a documented quality system that covers design, manufacturing, packaging, labeling, storage, installation, and servicing for finished devices intended for human use.
- Risk class still drives the route: Most Class I devices are exempt from 510(k), most Class II devices require 510(k), and most Class III devices usually require Premarket Approval.
- Materials are judged in context: The FDA evaluates the finished device and intended use, not a blanket approval for a material in every possible application.
- Validation is not optional: Build parameters, software workflow, material controls, post-processing, and sterilization all need evidence.
- Point-of-care printing adds complexity: When printing happens in a hospital or clinic, the facility, operator, file workflow, and release criteria become part of the manufacturing story.
- The field is already real: The FDA has cleared over 100 devices made using additive manufacturing technologies, which tells me the technology has moved well beyond experimentation.
I find the regulatory message fairly consistent: the more patient-specific, implantable, or clinically critical the part is, the more the process must look like a disciplined manufacturing program rather than a convenient local print job. Even when the paperwork is right, though, projects can still fail on technical details that teams underestimate.
Where programs usually break down
The weakest projects are usually not weak because the printer cannot print. They are weak because someone assumed that a clean-looking part was the same thing as a clinically safe, repeatable, releasable part.
- Prototype tolerance is treated as clinical tolerance: A model that looks accurate on a bench can still miss the fit or function needed in a patient.
- Sterilization gets bolted on too late: Heat, chemicals, or radiation can alter dimensions, surface texture, or mechanical performance.
- The material is chosen for printability instead of use: A resin or polymer that prints beautifully may still be a poor choice for bone contact, repeated cleaning, or load-bearing use.
- Layer direction is ignored: Build orientation affects strength. If the load path and layer path conflict, failure risk goes up.
- Traceability is incomplete: If the file version, powder lot, cure cycle, or machine settings cannot be traced, the part is much harder to defend.
- Fatigue and creep are underestimated: Fatigue is failure from repeated loading, and creep is slow deformation over time. Both matter a lot in medical parts that stay in service.
The biggest trap is treating additive manufacturing as a shortcut. It is usually the opposite. The technology removes tooling friction, but it adds process discipline. When a team respects that trade-off, the results are much better.
Before I would scale any medical printing program, I would run a short readiness check.
How I would judge whether a project is ready to scale
My first question is always whether the part truly benefits from customization. If the answer is no, conventional manufacturing may still be the better business and clinical choice. If the answer is yes, then I start looking at the quality chain.
- Is the device geometry genuinely patient-specific or functionally complex? If the answer is only “it looks cool,” the business case is probably weak.
- Can the imaging data be turned into a repeatable, controlled file? File quality is part of product quality.
- Is there a qualified material and post-processing route? The print is only as good as the full process around it.
- Do you know the intended contact, load, and sterilization method? Those three questions often determine the right material faster than any printer spec sheet.
- Can every build be traced from design through release? If not, scaling will be painful.
- Do you have a plan for machine drift and material variation? Medical production needs control over change, not just control over the first build.
If those answers are clear, the project starts to look scalable. If they are fuzzy, the right move is usually to slow down, tighten the validation plan, and avoid turning a promising prototype into a compliance problem. That is where the field is headed next.
What will matter next for printed medical parts
The next gains will come less from printers getting faster and more from the surrounding system getting smarter. Better segmentation software, better in-process monitoring, better traceability, and more standardized validation packages will do more for real-world adoption than another round of marketing about machine speed.
I also expect the most durable progress to happen where design, quality, and clinical workflow are connected early. Teams that involve surgeons, engineers, and quality specialists from the start usually make better choices about material, sterilization, and release criteria. That is especially true for implantable parts and hospital-based programs, where the line between design and manufacturing is thin.
The field is moving toward more patient-specific use, more sophisticated plastic and metal systems, and more disciplined regulation. The organizations that win will be the ones that treat additive manufacturing as a controlled medical process, not a novelty feature.